LIPODYSTROPHY
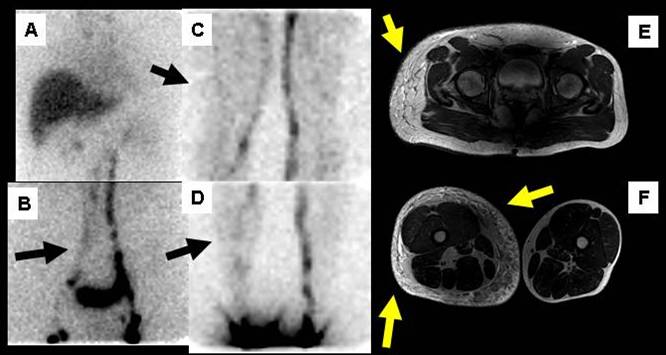
Male patient, 29 year old referred with diagnosis of lipodystrophy and right lower extremity lymphedema and genitalia. Asymmetric right thigh syndrome suspected Klippel-Trenaunay syndrome. Magnetic Resonance Angiography of the right thigh. Comparative examination. It has muscle MRI Examination before and after intravenous use gadolinium, with emphasis on venous phase sequences. The most striking finding is hypertrophy in subcutaneous thigh, associated with edema and signs of strengthening lobular septa, which extends along the entire thigh, with engagement of the pelvic girdle, which determines a marked asymmetry of the size of both thighs. Diagnostic impression: cellular hypertrophy subcutaneous region of the right thigh and pelvic girdle, asymmetrically distributed, associated with dilated veins in the right femoral triangle. Within the diagnostic differential should be considered a Klippel-Trenaunay syndrome.
Lymphoscintigraphy: Injection interdigital region between first and second toes on both feet with subdermal administration of the radiotracer. First is punctured the right foot. Sequential images were obtained from the feet to the thoracic region. The transit is normal in lymphatic pathways on the left leg. Numerous lymph nodes are seen at the level of inguinal and iliac path. On the right side there is slow flow, with faint visualization of the channels appearance of collateral lymphatic level leg and thigh, contrast of some inguinal lymph nodes and minimum lumboaórtica ascent to the region when is compared with the contralateral extremity. CONCLUSION: 1. - Study lymphedema of genital region and lower limb in right side. 2. - The findings suggest lumboaórtic obstruction and at pelvic level. 3. - Correlation is consistent with the clinical diagnosis of lipodystrophy.
Monnin-Delhom ED et al. evaluated the accuracy of computed tomography (CT) scan imaging in distinguishing lymphedema from deep venous thrombosis (DVT) and lipodystrophy (lipedema) in patients with swollen legs. Edema accumulation is readily demonstrated with plain CT scan and is not present in lipedema. Specific CT features of the subcutaneous fat and muscle compartments allow accurate differentiation between lymphedema and DVT (1).
Boursier V et al. demonstrated that in lower limb lymphoscintigraphy lymphatic insufficiency in lipedema without morphologic abnormality as seen in lymphedema. Lymphoscintigraphy is not indispensable but is a useful tool when diagnosis is doubtful (2).
References:
1 Monnin-Delhom ED, Gallix BP, Achard C, Bruel JM, Janbon C. High resolution unenhanced computed tomography in patients with swollen legs. Lymphology. 2002 Sep;35(3):121-8.
2
Boursier V, Pecking A, Vignes S. Comparative analysis of lymphoscintigraphy
between lipedema and lower limb lymphedema. J Mal Vasc. 2004 Dec;29(5):257-61.