Breast Sentinel Node (Prepared by Dr Isabel Berrocal)
51 year-old female
patient in preoperative assesment with sentinel node lymphoscintigraphy for
infiltrative left breast cancer.
Breast ultrasound showed a 25 x 17x 23 mm mass in the upper outer quadrant of
left breast and an ipsilateral axillary lymph node associated with 15 mm of
thickening. BIRADS 5.
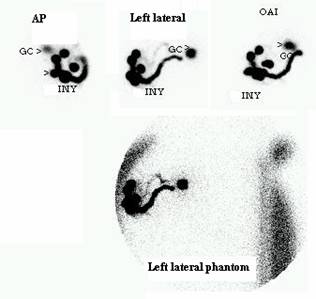
Lymphoscintigraphy with Tc 99m Nanocint, showed early contrast of tortuous
pathways to the axilla lymph node, which was marked on skin with china ink on
left lateral projection (GC). No activity in the contralateral internal mammary
chain was noted.
Lymphoscintigraphy
(LS) allows the surgeon to easily identify and biopsy the sentinel lymph node.
This method cannot determine if it is involved with cancer and also guides the
decision for the axillary lymph node dissection.
The sentinel lymph node biopsy is associated with less arm morbidity and better
quality of life than axillary lymph node dissection, when it is negative. Large
observational studies have shown that sentinel lymph node biopsy is associated
with low local recurrence rate and similar survival to axillary lymph node
dissection.
References:
1. Buscombe J., Paganelli G. Sentinel node in breast cancer procedural
guidelines. Eur J Nucl Med Mol Imaging (2007) 34:2154–2159.
2. Sicart V, et al. Scintigraphic and intraoperative detection of the sentinel
lymph node in breast cancer. Rev Esp Med Nucl. 2009 Jan-Feb;28(1):41-3.
3. Goyal A, Mansel R. Recent advances in sentinel lymph node biopsy for breast
cancer. Curr Opin Oncol. 2008 Nov;20(6):6216.