Bilateral kidney Tubular Injury Secondary to Cocaine Abuse
(Prepared by Dr Javiera Gonzalez)
Male, 43 year old, with a long history of cocaine use, about once a month. Refers 3 hours course of nausea, palpitations, vomiting, anxiety, headache and body aches, no chest pain. All symptoms began after consuming 3 grams of cocaine. At the moment of consultation BP 162/117 mmHg. HR 127 bpm. Myoglobin 699.3 ng/mL. Creatinine 2.34 mg/dL. Total CK 870 UI/L.
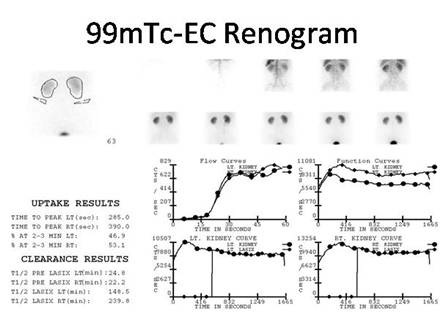
Both kidneys show preserved perfusion with normal uptake (upper graphs, time activity curves), however there is decreased excretion with bilateral retention and flat curves (lower graphs). This is consistent with diffuse parenchymal involvement secondary to ischemia, with a pattern similar to acute tubular necrosis. There is no pelvis nor ureteral dilation.
References:
1 Amoedo, M. Cocaine induced acute renal failure without rhabdomyolisis. Nefrol Dial Transplant 1999, 14:2971.
2 Mendoza, Asensi D. Acute renal insufficiency associated to cocaine consumption. Rev Clin Esp 204 (4): 206-211 2004.
3 Picazo Sánchez M. Cocaine use, high blood pressure and chronic kidney disease. Nefrologia 2010;30(6):706-707.
4 Machaiah M M. Acute bilateral renal infarction secondary to cocaine-induced vasospasm. Kidney Int 76: 576-580.
5
Furaz, K.C. Infarto renal e insuficiencia renal aguda por consumo de cocaína.
Nefrología 2008; 28 (3) 347-349.
Home
Index Clinical Applications
Kidney Function Assessment