Gastric Carcinoma
Male patient
38 year old presented with diagnosis of gastric cancer and liver metastases. Came
after 2 cycles of chemotherapy. Correlative Studies: Chest x-ray: no significant
findings. Abdominal ultrasound: mild hepatomegaly with multiple intraparenchymal
focal lesions. CT of the abdomen and pelvis: hepatomegaly multinodular
metastatic. Focal thickening of the stomach. Upper Endoscopy: gastric ulcer
lesion; prominent folds. Colonoscopy Ileoscopy: small internal
hemorrhoids. Stomach Biopsy: tubular adenocarcinoma moderately differentiated,
grade II ulceration and necrosis of Broders.
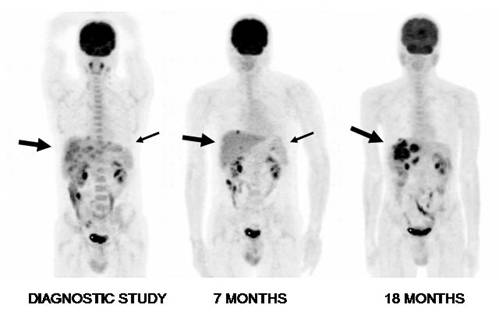
PET FDG Dose:
12 mCi, injected with glucose of 83 mg/dl shows a slightly enlarged liver with
multiple foci of moderate to intense increased uptake of FDG, distributed in
both lobes, with sizes ranging from 1.5 cm to 4.5 cm, several of them confluent,
especially in the right lobe (large arrow), consistent with metastatic lesions. There is diffuse increased tracer
activity in skeletal bone marrow, explainable by recent chemotherapy. In the
stomach, there is diffuse uptake and irregular, with most intense contrast, anteriorly
(small arrow) and
correlates with a primary malignant lesion under chemotherapy. In the remainder of the study, normal distribution is observed
in brain, spleen, colon, kidney and bladder.
Seven months later and after completing chemotherapy, there is evidence of significant metabolic response to treatment, with persistent small liver foci and mild gastric activity. There were no new abnormal hypermetabolic foci. A gastric total resection was conducted including the primary tumor.
Eighteen months later, multiple areas are seen with intense FDG uptake in liver, some confluent, especially in the dome, progressing in number and size of nodules compared to previous examination from a year ago and indicating worsening of the malignant condition.
This case demonstrates that F18-FDG, was adequate at the initial diagnosis and for follow up.
Sharma P. et al found that out of 93 PET-CT studies, 56 (60.2%) were positive
and 37 (39.8%) were negative for recurrent disease. On per-study-based analysis,
F18-FDG PET-CT has a sensitivity, specificity and accuracy of 95.9, 79.5 and
88.1%, respectively. The accuracy of F-FDG PET-CT was 89.2% for local
recurrence, 94.6% for lymph nodes, 96.7% for liver, 96.7% for lung, 98.9% for
bone and 98.9% for other sites. The accuracy of F18-FDG PET-CT was lower for
local recurrence as compared with that for liver (P=0.012) and bone (P=0.012).
No significant difference was found in the diagnostic accuracies for other
regions.
References:
1 Sharma P, Singh H, Suman SK,
Sharma A, Reddy RM, Thulkar S, Bal C, Malhotra A, Kumar R. 18F-FDG PET-CT for
detecting recurrent gastric adenocarcinoma: results from a Non-Oriental Asian
population. Nucl Med Commun. 2012 Sep;33(9):960-6.
Home
Index
18F-FDG Tumor Imaging
Clinical Applications