Rectosigmoid Cancer and Peritoneal Carcinomatosis
Patient 49
year old with a history of cancer colorectal cancer T4N2M0 stage IIIB. Underwent rectosigmoid surgery.
Followed by radiation therapy and chemotherapy. Currently,
presents with prominent abdomen. Correlative studies: CT, abdomen and pelvis: horseshoe kidneyt, right pelvic cystic
mass, probably ovarian. Abdominal ultrasound: cholelithiasis; ascites. Chest X-ray:
atelectasis of lung bases, bilateral pleural effusion.
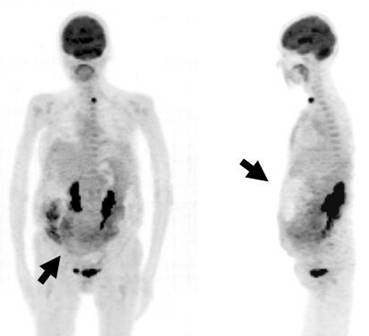
On the PET, there
is abdominal and diaphragm distension explained by ascites (arrow in the
right hand side image), associated
with diffuse increased FDG fixation in abdominal contour, more evident activity in
the right flank (arrow, on left hand side image).
Furthermore, a moderate intensity focus in the lower anterior inferior abdominal region.
Additionally a focus of intense tracer uptake in lower anterior cervical region
in the left thyroid lobe of 1.7 cm diameter.
In the remainder of the study, normal distribution is observed in brain, lung,
liver, spleen, colon and bladder. Kidneys have pyelocaliceal dilation.
The findings described in abdominal cavity are compatible with peritoneal
carcinomatosis.
The left thyroid lobe nodule suggests a malignant lesion and should be correlated with additional tests
including a biopsy.
Despite its known limited accuracy in detecting small peritoneal lesions and the involvement of the small bowel/mesentery, contrast-enhanced MDCT remains the standard imaging modality in the assessment of peritoneal carcinomatosis. MRI, especially with diffusion-weighted images, and FDG-PET/CT are promising methods for the evaluation of peritoneal carcinomatosis with superior results in recent studies, but still have a limited role in selected cases because of high costs and limited availability (3).
Contrast-enhanced, multidetector computed tomography scan remains the
standard imaging modality in the assessment of peritoneal carcinomatosis.
Magnetic resonance imaging may offer complementary valuable data. Positron
emission tomography (PET) has a more limited role, its main indication
being the detection of unsuspected extraperitoneal involvement in nonmucinous
neoplasms (4).
References:
1 Culverwell AD, Chowdhury FU, Scarsbrook AF. Optimizing the role of FDG PET-CT for potentially operable metastatic colorectal cancer.Abdom Imaging. 2012 Feb 28.
2 Ozkan E, Soydal C, Araz M, Kir KM, Ibis E. The role of 18F-FDG PET/CT in detecting colorectal cancer recurrence in patients with elevated CEA levels. Nucl Med Commun. 2012 Apr;33(4):395-402.
3 Pfannenberg C, Schwenzer NF, Bruecher BL. State-of-the-art imaging of peritoneal carcinomatosis. Rofo. 2012 Mar;184(3):205-13.
4 González-Moreno S, González-Bayón L, Ortega-Pérez G, González-Hernando C. Imaging of peritoneal carcinomatosis. Cancer J. 2009 May-Jun;15(3):184-9.