Head Pancreatic Carcinoma
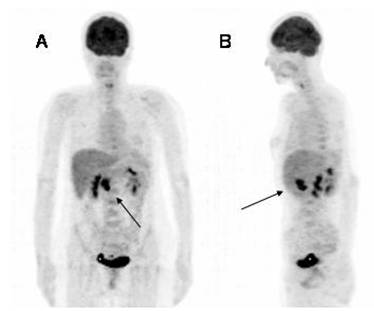
Female, 48 year old patient with a history of pancreatic head tumor diagnosed by CT and MRI (not shown). She was referred for initial staging. There is 18F-FDG PET hypermetabolic activity in the right epigastrium compatible with a malignant tumor of the pancreas head (Volumetric images, A (frontal) and B (right lateral), black arrows) (SUVmáx of 10.5), without other locations.
From the anatomical point of view pancreas cancer is located in the head in 78%, in the body in 11% andin the tail in 11% .
In the literature it is described low uptake of mucinous cystadenoma due to its low cellularity, often being a false negative. Intraductal papillary mucinous tumor would concentrate in a variable way and according to its degree of malignancy, as well as solid pseudo papillary tumor. In the latter, Nakagohri et al. described an average SUV of 6.3, range 0.9-42.8. On the other hand, ductal adenocarcinoma and acinar cell carcinoma would show intense uptake.
18F-FDG PET/CT is recognized as a useful tool in the preoperative diagnosis of pancreas cancer, since the correlation between FDG focal uptake and the anatomy modality for location reduces false positives. Heinrich et al. prospectively studied 59 patients with PET-FDG/CT with hybrid machine for detecting pancreatic lesions, with a sensitivity of 89%, specificity of 69%, PPV of 91% and NPV of 64%. These data corroborate those found by Lemke et al., in which studied 104 patients with fused images PET-FDG/CT for diagnosing pancreatic malignancy found a sensitivity of 89%, specificity of 64%, PPV of 81% and NPV of 76%.
References:
1 Heinrich S, Goerres GW, Schäfer M, Sagmeister M, Bauerfeind P, Pestalozzi BC, Hany TF, von Schulthess GK, Clavien PA. Positron emission tomography/computed tomography influences on the management of resectable pancreatic cancer and its cost-effectiveness. Ann Surg. 2005 Aug;242(2):235-43.
2 Lemke AJ, Niehues SM, Hosten N, Amthauer H, Boehmig M, Stroszczynski C, Rohlfing T, Rosewicz S, Felix R. Retrospective digital image fusion of multidetector CT and 18F-FDG PET: clinical value in pancreatic lesions--a prospective study with 104 patients. J Nucl Med. 2004 Aug;45(8):1279-86.
3
Lachter J, Adler AC, Keidar Z, Haddad R. FDG-PET/CT identifies a curable
pancreatic cancer surgical tract metastasis after
failure by other imaging modalities. Isr Med Assoc J. 2008 Mar;10(3):243-4.
4 Saif
MW, Cornfeld D, Modarresifar H, Ojha B. 18F-FDG positron emission tomography CT
(FDG PET-CT) in the management of
pancreatic cancer: initial experience in 12 patients. J Gastrointestin Liver
Dis. 2008 Jun;17(2):173-8.
5 Kitajima K, Murakami K, Yamasaki E, Kaji Y, Shimoda M, Kubota K, Suganuma N, Sugimura K. Performance of integrated FDG-PET/contrast-enhanced CT in the diagnosis of recurrent pancreatic cancer: comparison with integrated FDG-PET/non-contrast-enhanced CT and enhanced CT. Mol Imaging Biol. 2010 Aug;12(4):452-9.
6 Strobel K, Heinrich S, Bhure U, Soyka J, Veit-Haibach P, Pestalozzi BC, Clavien PA, Hany TF.Contrast-enhanced 18F-FDG PET/CT: 1-stop-shop imaging for assessing the resectability of pancreatic cancer.J Nucl Med. 2008 Sep;49(9):1408-13.
7
Nakagohri T, Kinoshita T, Konishi M, Takahashi S, Gotohda N. Surgical outcome of
solid pseudopapillary tumor of the pancreas. J Hepatobiliary Pancreat Surg.
2008;15(3):318-21.