(Prepared by Dr Jaime Carmona)
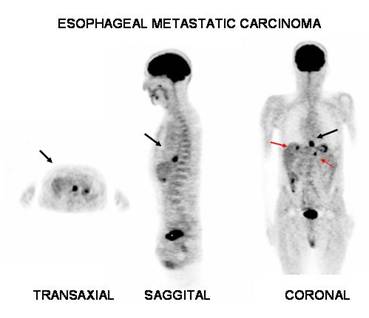
Male, 60 year old, with history of esophageal cancer (squamous cell carcinoma partially differentiated grade II to III Broders). PET-FDG with 12mCi, injected with blood glucose level of 63 mg/dl showed intense tracer uptake in the distal third of the esophagus that measures approximately 28 mm, with maximum SUV of 13.8 (black arrows). In addition, a second focus of concentration of FDG in the right hepatic lobe measuring 16 mm with maximum SUV of 4.9 and another one in the lateral aspect of the left liver lobe size 11 mm with maximum SUV of 4.8 (red arrows).
Himeno et al found that "PET imaging can detect primary esophageal cancer with a depth of invasion of T1b or greater, but Tis and T1a tumors are undetectable. PET seems to be more accurate than CT or EUS for diagnosing lymph node metastasis" (1).
Guo et al commented that "FDG
PET/CT is highly effective for detecting recurrent ESCC (esophageal squamous
cell carcinoma). The relatively low specificity at local sites is associated
primarily with a high rate of false-positive interpretations at anastomoses.
PET/CT can also provide noninvasive and independent prognostic information using
SUV and recurrent disease pattern on PET/CT images for previously treated ESCC"
(3).
References:
1 Himeno S, Yasuda S, Shimada H, Tajima T, Makuuchi H. Evaluation of esophageal cancer by positron emission tomography. Jpn J Clin Oncol. 2002 Sep;32(9):340-6.
2 Rohren EM, Turkington TG, Coleman RE. Clinical applications of PET in oncology. Radiology. 2004 May; 231(2): 305-32.
3 Guo H, Zhu H, Xi Y, Zhang B, Li L, Huang Y, Zhang J, Fu Z, Yang G, Yuan S, Yu J.Diagnostic and prognostic value of 18F-FDG PET/CT for patients with suspected recurrence from squamous cell carcinoma of the esophagus. J Nucl Med. 2007 Aug;48(8):1251-8.