BROWN FAT ON FDG PET-CT
(Collaboration of Dr JUAN PABLO ZHINDON)
Adipose tissue is presented in most mammals in two varieties, which differ by their color, distribution, metabolism and vascularization activity in white fat and brown fat. White adipose tissue is the most body fat component. The hibernoma is a rare benign tumor composed of brown fat. The range of brown adipose tissue is found only in parts of the body and stored, providing insulation against heat loss. Brown fat also plays a metabolic function, to ensure the storage of energy reserves. The region with the largest amount of brown fat in fetuses and newborns is the retroperitoneum, and decreases from 2 months of vida.Comparado with white fat, the brown adipose tissue has smaller cells of different size, aspect multilocular. The greater number of mitochondria present in brown fat is related to the exothermic function of this tissue, which is a unique property pardo.Asimismo adipose tissue, connective tissue surrounding these cells is low and has good blood supply, which hypervascular characteristics conferred on imaging studies.
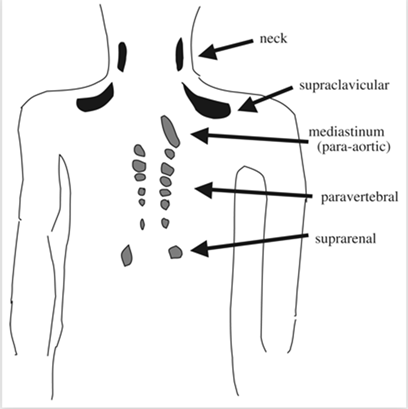
Sites of FDG uptake corresponding to brown adipose tissue in adult humans. The black areas are those that are most frequently described; the gray areas are not always found.
Male, 32 years old who comes to see the doctor for a lump with no pain in the right supraclavicular region, 10 months coyrse. Physical examination reveals right supraclavicular soft mass, 6 cm in diameter . Computed tomography demonstrated a space occupying lesion in the base of the neck, ¿ malignant schwanoma ?. Magnetic resonance also showed a tumor in the same location ¿ neurogenic sarcoma ?.
At PET with computed tomography it could be seen a hypermetabolic mass. in the right side with no signs of dissemination. See below MIP projection (top left and fusion image, bottom right).
Biopsy was consistent with hibernoma.

The hibernoma is a rare tumor and has been reported more frequently in the third and fourth decades of life, with no gender predominance. Clinically, it manifests as a mobile palpable mass, usually in the extremities, with slow and painless growth. Can be found simultaneously in several locations. No cases of metastasis or local recurrence after surgical excision communicate.
Other differential diagnoses uncommon to consider are myxoid liposacorma, angiomyolipoma and myxoid liposarcoma mesentérica. Panniculitis may present a clinical picture similar to hibernoma and lipoblastoma radiological findings, but is associated with an infiltrative growth, cellular atypia and presents extremely rare in children.
The hibernomas do not have specific characteristics by imaging methods. On ultrasound echogenic, heterogeneous formations are demonstrated, showing vascular flow with Doppler color. In most cases, for a better characterization, CT or magnetic resonance imaging (MRI) is needed. The latter, with some particular fat suppression sequences, providing conclusive identification data of the fat component. MRI and a PET scan alone can rarely supply the diagnosis of hibernoma when faced with a fatty tumour. On the other hand, the combination of data from these two examinations (FDG hyperfixation and T1-weighted hypointensity relative to subcutaneous fat) can increase diagnostic certainty and make a biopsy less systematic.
References:
1 Bauwens M, Wierts R, van Royen B, Bucerius J, Backes W, Mottaghy F, Brans B. Molecular imaging of brown adipose tissue in health and disease. Eur J Nucl Med Mol Imaging. 2014 Apr;41(4):776-91.
2 Hao R, Yuan L, Zhang N, Li C, Yang J. Brown adipose tissue: distribution and influencing factors on FDG PET/CT scan.
J Pediatr Endocrinol Metab. 2012;25(3-4):233-7.
3 Ognong Boulemo A, Roch JA, Ricard F, Fontaine Hommell J, Cotton F.
Hibernoma: don't be caught out by a PET scan!. Diagn Interv Imaging. 2013 Jun;94(6):649-51.