Bone Scan Spondylodiscitis
35 y/o, male, with
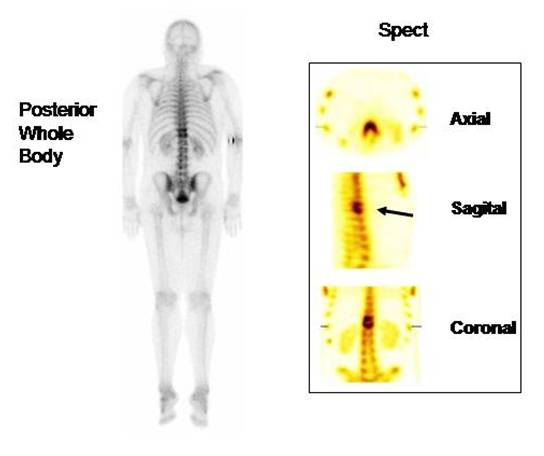
3 week back pain and intermitent fever. The Tc99m MDP bone scan showed increase
bone uptake in T11-T12 but it wasnt clear to show vertebral body involvement.
SPECT confirmed intense increase uptake in the vertebral bodies. Note "sandwich
appearance". (arrow).
Infectious spondylodiscitis was confirmed surgically. Patient underwent
immediate debridement of the focus, with decompression, stabilization and
antibiotic therapy.
(Prepared by Dr Gabriel Castro )
Often the signs and symptoms of spondylodiscitis are vague and therefore the
diagnosis may be delayed. Radiographic changes are inespecific and do not
usually appear until two weeks after infection (1). The most frequent disease
germs are Staphylococcus aureus (60%), Enterobacter (30%), more rarely
Escherichia coli, Salmonella, Pseudomonas aeruginosa and Klebsiella pneumoniae
(2).
Bone scintigraphy is a valuable diagnostic (90% sensitivity) procedure for
discitis, with earlier detection than plain radiography and similar initial
detection to that of computed tomography. Single photon emission computed
tomographic imaging increases diagnostic specificity (3).
References:
1) Nolla-Solé J et al. Role of technetium-99m diphosphonate and gallium-67
citrate bone scanning in the early diagnosis of infectious spondylodiscitis. A
comparative study. Ann Rheum Dis 1992; 51: 665-667.
2) Stanislaw Pilecki et al.The role of radioisotopic methods in imaging of
intervertebral disc inflammation in children. Nucl Med Rev 2006 Vol. 9, No. 1,
pp. 72-76.
3) Choong K,Monaghan P.Role of bone scintigraphy in the early diagnosis of
discitis. Ann Rheum Dis. 1990 Nov;49(11): 932-4.
Home Index Clinical Applications Clinical Applications Infections