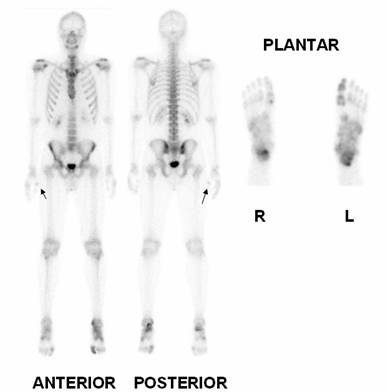
Psoriatic Arthritis
Male 26 year old, complains of joint pain mainly in the feet. He was referred for a bone scan with diagnosis of psoriatic arthritis. Note increased uptake in first right metacarpophalangeal joint (arrows ), shoulders, both sacroiliac joints especially in the right side, knees, both tarsi, left ankle, in the two calcaneal (plantar view is very demonstrative), several small joints in toes, being more evident in the first one of the left side. Sacroiliac Index was 1.3 in the right side and 1.1 in the left one. Normal renal excretion.
Psoriatic arthritis is part of the group of seronegative spondyloarthropathies as ankylosing spondylitis, Reiter's disease, enteropathic spondylitis, and undifferentiated spondyloarthropathy. All of these diseases share common clinical and radiographic features with characteristic involvement of the sacroiliac joints, spine, and to various degrees, the peripheral joints (1).
It has been described five clinical patterns of joint involvement in psoriatic arthritis: 1) distal arthritis (involvement of the DIP joints), 2) asymmetric oligoarthritis, 3) symmetric polyarthritis, 4) arthritis mutilans, and 5) spondyloarthropathy. Distal arthritis and arthritis mutilans are specific for psoriatic arthritis (2).
Imaging modalities including bone scintigraphy, and computed tomography, have improved visualization of inflammatory changes at the sacroiliac joints. Magnetic resonance by directly imaging the synovium, articular cartilage, and subchondral bone, is sensitive and specific for sacroiliitis (1).
Three patterns of bone involvement can be differentiated in psoriatic arthritis distal, central, and distal combined with central. Distal involvement is more specific for psoriatic arthritis, with radial and/or transverse involvement of the distal interphalangeal joints. Psoriatic arthritis originates in the periarticular bone and extends towards the synovia, whereas in
rheumatoid arthritis it extends in the opposite direction. Bone scintigraphy is sensitive in the diagnosis of psoriatic bone involvement with documentation of specific patterns and presence of disease in multiple sites (3).Seronegative arthritis can also cause enthesopathies that produce heel pain and should be considered in a differential diagnosis list (4). Also spondylodiscitis may be the only manifestation of the onset of psoriatic spondyloarthritis, which can be detected by MRI , CT and Bone Scan (5).
References:
1. Luong AA, Salonen DC. Imaging of the seronegative spondyloarthropathies. Curr Rheumatol Rep. 2000 Aug;2(4):288-96.Lee KH, Son MK, Ha YJ, Choi ST, Lee SW, Park YB, Lee SK. Inflammatory polyarthritis in a patient with psoriasis: is it psoriatic arthritis or rheumatoid arthritis?. Korean J Intern Med. 2010 Jun;25(2):224-6.
3 Holzmann H, Krause BJ, Kaltwasser JP, Werner RJ. Psoriatic osteoarthropathy and bone scintigraphy. Hautarzt. 1996 Jun;47(6):427-31.
4 Yedon DF, Howitt S. Heel pain due to psoriatic arthritis in a 50 year old recreational male athlete: case report. J Can Chiropr Assoc. 2011 Dec;55(4):288-93.
5 Bruzzese V. Spondylodiscitis as the only clinical manifestation of the onset of psoriatic spondyloarthritis. Reumatismo. 2011 Mar;63(1):38-43.
6 Mejjad O, Daragon A, Louvel JP, Da Silva LF, Thomine E, Lauret P, Le Loët X. Osteoarticular manifestations of pustulosis palmaris et plantaris and of psoriasis: two distinct entities. Ann Rheum Dis. 1996 Mar;55(3):177-80.
Home Index Clinical Applications Clinical Applications Inflammatory